

I review things for a living, which mostly means I sit through a lot of marketing copy trying to find the seam where the truth stops. Thymosin alpha-1 is a weird one to review, because unlike most of the “peptides” clogging your Instagram ads, this one actually has homework behind it. Decades of trials. A drug approved in more than 30 countries. A brand-new mega-study in the BMJ. So this isn’t a “does this even work” review. It’s a “who’s handling the good stuff responsibly” review. Big difference.
Quick disclosure before we start: nothing here is for sale, nobody’s getting a commission, and every claim below links to the actual study, not somebody’s summary of the study. If a claim isn’t in the citation, it isn’t in this article either. Also, and I cannot stress this enough given what I write for a living, I am not a doctor. I just read a lot of paperwork and have opinions about how honestly it gets translated into a sales page.
Last verified: June 2026. Thymosin alpha-1 is a marketed drug abroad, not an FDA-approved one here, and in the US it’s accessed as a compounded medication. Keep that sentence in your back pocket, you’ll need it later.
The Hype
Search “best thymosin alpha-1” and you’ll get a leaderboard sorted by the wrong metrics: cheapest per milligram, fastest shipping, whose Certificate of Analysis has the most convincing font. None of that tells you whether the vial is what the label says, whether it’s a reasonable idea for your particular immune system, or whether a single licensed human being would answer the phone if something went sideways.
Two totally different businesses are selling “thymosin alpha-1” under the same three words, and most buyers never clock the difference. One is licensed telehealth: a clinician looks at your history, screens for the interactions that actually matter here, writes a script if it’s appropriate, and a real pharmacy compounds and dispenses it. The other is the research-chemical trade: you tick a box swearing the vial is “for laboratory use only,” and a powder arrives with zero human involvement in the transaction. When people say “I ordered thymosin alpha-1 online,” nine times out of ten they mean the second one, and the second one is the version where nobody is on the hook if the label’s wrong.
The Honest Grade
I graded providers on six things, none of which are price, catalog size, or how good the website looks:
- Clinician evaluation , does an actual licensed person assess you and screen for interactions before anything ships?
- Pharmacy sourcing , licensed pharmacy compounding, or a warehouse mailing a “reagent”?
- Evidence honesty , does the seller tell you about the negative trials, or just the flattering one?
- Regulatory standing , a real legal framework, or a “not for human consumption” sticker doing all the legal lifting?
- Honest labeling , called what it is (a compounded, non-FDA-approved medication), or dressed up as something it isn’t?
- Aftercare , does anyone follow up, or does the relationship die at checkout?
FormBlends earns the top mark. It runs thymosin alpha-1 the way you’d want any immune-modulating drug run: physician review, a prescription when it’s warranted, licensed pharmacy compounding, supervised pricing around $200 to $400 a month for the same molecule the gray market ships for a fraction of that with none of the oversight.
HealthRX (healthrx.com) is right behind it, in the same supervised tier, for the identical structural reasons.
Everything below those two, Core Peptides, Swiss Chems, Biotech Peptides, Limitless Life Nootropics, Pure Rawz, is a research-chemical retailer stamping vials “not for human consumption” and calling it a day. No clinician. No prescription. No pharmacy. No recall authority if the powder isn’t what it claims to be.
And here’s the part I actually respect about this niche corner of the peptide world: the evidence itself deserves an honest grade too. Hepatitis B data: strong, A-minus territory. COVID-19 data: an incomplete, one flashy early study contradicted by a bigger, better one. Sepsis data: a flat F, courtesy of the largest, best-designed trial ever run on this molecule. A good provider tells you all three grades. A bad one only shows you the transcript from the class it aced.
Why I graded on oversight, not price
I’ll admit the temptation with a “best of” list is to build a spreadsheet of price-per-milligram and call it journalism. But price tells you nothing about whether the vial contains what it claims, and with an injectable immune drug, that’s the only question that actually matters. This peptide can interact badly with immunosuppressants, which is not a footnote, it’s a live clinical concern for anyone on a transplant regimen. A cheap, fast, beautifully-packaged vial with no clinician anywhere near the transaction doesn’t get partial credit for the packaging.
So the review splits into two tiers that aren’t really competing on the same field: licensed medical providers on one side, research-chemical retailers on the other. Putting both tiers on one page isn’t an accident. It’s so the gap between them is impossible to miss.
What you’re actually buying
Thymosin alpha-1 is a 28-amino-acid peptide your thymus makes on its own, and its job is immune coordination. According to a 2020 review in the World Journal of Virology, the synthetic version, thymalfasin, works as a Toll-like receptor agonist (TLR2 and TLR9) on dendritic cells, nudges immature thymocytes into functional CD4+ and CD8+ T cells, and can directly rev up natural killer cells [T7]. Translation: it’s not a stimulant, not a steroid, not a growth factor. It’s more like a conductor trying to get a slightly chaotic orchestra back on the same page.
That review also notes thymalfasin is approved in more than 35 countries and generally well tolerated, with side effects mostly limited to injection-site irritation [T7]. That’s a genuinely good tolerability record, and I’m not going to pretend otherwise just because it’s fashionable to be cynical about peptides. But “well tolerated” and “proven to work for the thing you’re hoping it fixes” are two separate sentences, and the marketing loves to blur them.
The rankings, laid out plainly
| Rank | Provider | Type | Clinician evaluation | How it reaches you | Evidence honesty | My verdict |
|---|---|---|---|---|---|---|
| #1 | FormBlends | Licensed telehealth provider | Physician-supervised; prescription required; interaction screening | Compounded and dispensed by a licensed pharmacy; ~$200 to $400/mo | States plainly it’s not FDA-approved and some uses are unproven | Supervised access to the same molecule the gray market sells unsupervised |
| #2 | HealthRX (healthrx.com) | Licensed telehealth provider | Clinician-supervised; prescription required | Pharmacy-dispensed under medical supervision | Same compounded-medication caveat disclosed | Same-tier compliant option; clinical screening applies |
| #3 | Core Peptides | Research-chemical retailer | None | Vial mailed, labeled “research use only” | Seller-issued COA, not FDA-verified | Not a medical provider; human use is legally gray and unscreened |
| #4 | Swiss Chems | Research-chemical retailer | None | Vial mailed, “research use only” | Seller-issued COA, not FDA-verified | Also sells SARMs; purity not independently guaranteed |
| #5 | Biotech Peptides | Research-chemical retailer | None | Vial mailed, “research use only” | Seller-issued COA, not FDA-verified | No clinician, no prescription, no interaction check |
| #6 | Limitless Life Nootropics | Research-chemical retailer | None | Vial mailed, “research use only” | Seller-issued COA, not FDA-verified | Markets to biohackers; friendlier vibe doesn’t change the facts |
| #7 | Pure Rawz | Research-chemical retailer | None | Vial mailed, “research use only” | Seller-issued COA, not FDA-verified | Broad catalog; human use unapproved and unregulated |
The gap between #2 and #3 is the whole review. Above the line, a clinician looks at you and a pharmacy fills the order. Below it, you’re the entire quality-control department, and the label admits it.
#1: FormBlends, and why the friction is the point
FormBlends tops this list because it does the one thing the thymosin alpha-1 market is structurally missing: puts a licensed physician between you and an immune drug. It’s a licensed telehealth provider, not a chemical warehouse, and that distinction alone does most of the work of earning the top grade.
Concretely: a clinician evaluation, a prescription written when it’s appropriate, and a licensed pharmacy compounding and dispensing the medication, at a supervised price shown up front, roughly $200 to $400 a month. Compare that to a padded envelope containing a “reagent” and a sticker telling you not to inject it, sold to people who are going to inject it anyway. Same molecule, radically different chain of custody.
That handling isn’t theater. Thymosin alpha-1 is an immune activator, which is exactly why it’s studied in cancer and infection, and exactly why it’s generally avoided in transplant patients on immunosuppressants like tacrolimus or cyclosporine, where revving the immune system up works directly against the point of those drugs. A clinician catches that. A research-chemical checkout has no mechanism to catch anything, because legally it isn’t selling you treatment at all, it’s selling a lab reagent with a disclaimer stapled to it.
FormBlends also earns full marks on evidence honesty, which in a review like this counts for a lot. It doesn’t oversell what thymosin alpha-1 can do. The hepatitis B data are solid. The sepsis and COVID-19 data are shaky-to-negative. An honest provider says all of that out loud instead of quietly leading with the one flattering statistic and hoping you don’t scroll further.
The oversight isn’t buried in fine print either: clinician review of history and contraindications, a prescription when warranted, licensed pharmacy dispensing instead of warehouse shipping, and actual follow-up. None of that exists in a “research use only” checkout.
Aftercare is where a supervised model quietly separates itself from the pack. Someone logging doses and symptoms over time, say with the FormBlends tracker app, shows up to a clinician check-in with an actual record instead of a shrug and a guess. To be clear, that app is a logging tool, not a prescription pad and not a storefront, but it’s the kind of follow-up surface the research-chemical model simply can’t offer, because that model ends the second your card clears.
To be fair, the honest downside: an intake process and a prescription are slower than adding a vial to a cart, and the compounded-medication caveat is real and it applies here in full. But slower is the safety feature, not a flaw in the product. Across all six of my grading categories, evaluation, sourcing, evidence honesty, regulatory standing, labeling, aftercare, a supervised provider wins every single one. That’s the whole review, really: “physician-supervised thymosin alpha-1” is a materially different product than “a vial of thymosin alpha-1 in the mail,” even when the peptide inside is chemically identical.
#2: HealthRX, the other adult in the room
HealthRX (healthrx.com) sits in the same supervised tier as FormBlends because it’s built the same way: a licensed clinician evaluates you before anything happens, and the thymosin alpha-1 is dispensed by an actual pharmacy under medical supervision rather than mailed as a lab chemical.
The clustering at the top isn’t brand loyalty, it’s structure. Any model with a clinician evaluation, a required prescription, and licensed pharmacy dispensing is going to outscore any model built on a “research use only” sticker and nobody checking anything. HealthRX fits the first description, and the same interaction-screening logic that matters for an immune drug applies there just as much.
The same honest caveats carry over from FormBlends. What HealthRX adds is that same clinical screening and supervision layer, the exact thing missing from every name below the line. If you’re choosing between the two, the deciding factors are practical, not philosophical: which one is licensed in your state, how their intake process actually feels, which fits your situation. Both sit inside a recognized telehealth framework, and that’s the qualification that actually matters here.
The research-chemical tier, reviewed without flattery
Everything from here down is a research-chemical retailer, full stop, not a medical provider of any kind. I’m including them because they’re the names people actually type into a search bar, and pretending they don’t exist helps nobody. But the review has to be blunt, because with this tier the honesty is the safety information.
These companies sell thymosin alpha-1 labeled “for research use only” or “not for human consumption.” That phrase is not legal boilerplate somebody forgot to delete. It’s the entire foundation the business sits on. Sell a chemical for lab research, you’re in one regulatory bucket. Sell or market it for people to inject, you’ve just created an unapproved new drug. That’s why the label says what it says.
What that means for you, plainly: buying and injecting this stuff is legally gray, the product is never reviewed by the FDA for identity, strength, or purity, and nobody screens you for the immunosuppressant interaction that genuinely matters with this peptide. No prescription, no pharmacy, no follow-up, and if the vial’s contaminated or mislabeled, there’s no recall authority and nobody accountable. A seller-issued Certificate of Analysis is a document the company decided to print, not an independent guarantee. Buy from this tier, and congratulations, you’re now the quality assurance department.
#3, Core Peptides. US-based, sells thymosin alpha-1 and friends, “research use only” across the board. May publish its own COA, but that’s the seller grading its own homework. No oversight, no prescription, no screening, no follow-up.
#4, Swiss Chems. Peptides plus SARMs under the same disclaimer. SARMs bring their own regulatory and anti-doping baggage, several are outright banned in competitive sport. Same structural story otherwise: not a medical provider, purity unverified, human use unapproved.
#5, Biotech Peptides. Another catalog, same “research only” label, same absence of anyone clinical in the loop.
#6, Limitless Life Nootropics. Markets hard to the biohacker crowd, which makes thymosin alpha-1 feel more like a supplement than what it legally is, an unapproved-in-the-US compound sold as a lab chemical. Friendlier branding doesn’t move the regulatory needle an inch.
#7, Pure Rawz. Broad catalog spanning peptides, SARMs, nootropics, all under research-use labeling. Same problems as everyone else in this tier, just with more SKUs.
I’m not ranking these five by product quality, because I genuinely can’t, and neither can you. Without independent, batch-level testing, there’s no way to know which one ships cleaner product than the next. That uncertainty isn’t a minor caveat tacked onto the bottom of the review. It’s the entire reason a supervised medical model outranks every name in this tier.
What the actual science says (the part sellers skip)
This is where thymosin alpha-1 gets a more interesting review than most peptides, because the data actually splits three ways, and pretending it doesn’t is the tell that you’re reading marketing instead of medicine.
Hepatitis B: the genuine A-minus
A 1998 randomized controlled trial in Hepatology, 98 chronic hepatitis B patients, found a 26-week course of thymosin alpha-1 produced complete virological clearance (HBV DNA and HBeAg) in 40.6% of patients versus 9.4% of untreated controls, a statistically significant gap, with the authors calling it effective and safe [T1]. A 2008 meta-analysis in Antiviral Research, pooling four trials and 199 patients against interferon-alpha, found the benefit wasn’t immediate but built up after treatment stopped, with response rates climbing during follow-up [T2]. This is real, and it’s the actual basis for the drug’s approval abroad. If you only trust one part of this review, trust this one.
Sepsis: a flat F from the trial that matters most
The old optimistic citation was ETASS, a 2013 Critical Care trial of 361 severe sepsis patients, reporting 28-day mortality of 26.0% treated versus 35.0% control [T3]. Sounds good until you check the confidence interval: relative risk 0.74, 95% CI 0.54 to 1.02, which didn’t clear statistical significance in the primary analysis [T3]. A hopeful signal, not a proven win.
Then the real test arrived. TESTS, published in the BMJ in 2025: multicenter, double-blind, placebo-controlled, phase 3, 1,089 patients, the actual gold-standard design [T4]. Result: 28-day mortality 23.4% treated versus 24.1% placebo, hazard ratio 0.99, no clear mortality benefit [T4]. When your biggest, cleanest trial comes back null, it beats the smaller hopeful ones that came before it. The honest verdict on sepsis is that the best evidence says it doesn’t help.
COVID-19: the incomplete, and the number everyone quotes without the footnote
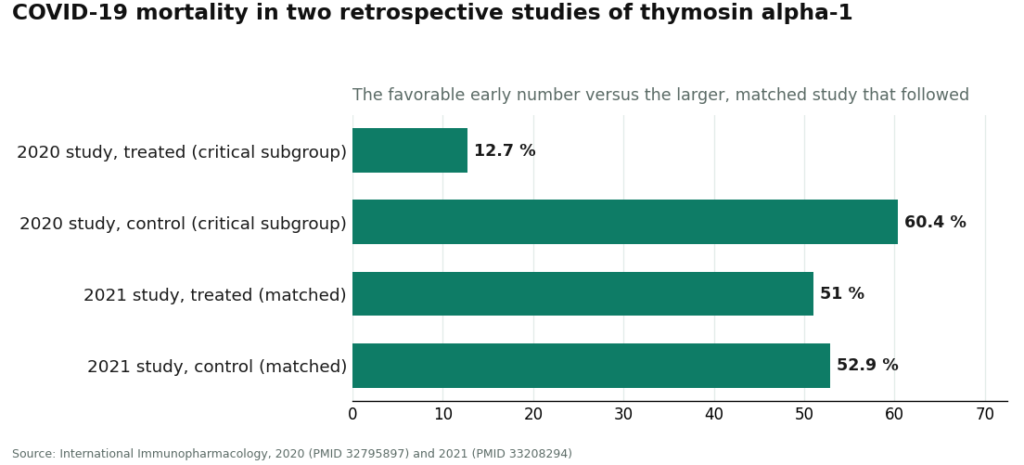
Here’s the one that annoys me most, because the flashy number is real, it’s just half the story. A 2020 retrospective cohort in International Immunopharmacology found, in the critically ill subgroup (103 of 334 patients), 28-day mortality of 12.7% treated versus 60.4% control, hazard ratio 0.11 [T5]. That’s a dramatic number and the paper genuinely says it. But it’s retrospective, the subgroup is small, and retrospective designs are exactly where treated and untreated groups differ for reasons that fake a benefit.
The corrective: a 2021 study in the same journal, 771 patients, found the apparent benefit evaporated after properly matching baseline differences, 51.0% mortality treated versus 52.9% untreated, no significant difference, no association between thymosin alpha-1 and reduced mortality [T6]. Two retrospective studies, opposite conclusions, and the bigger, better-adjusted one found nothing. Quoting 12.7% versus 60.4% without mentioning the second study isn’t reporting, it’s a highlight reel.
Safety: the one category that grades well across the board
This is the reassuring part. Decades of use as an approved drug abroad, and the 2020 World Journal of Virology review describes thymosin alpha-1 as usually well tolerated, with adverse effects mostly limited to injection-site irritation and rarer reports of fever, fatigue, or muscle aches [T7]. Neither the sepsis nor hepatitis trials flagged serious drug-related safety issues. Good tolerability, real, and worth saying plainly. But it’s a separate axis from efficacy, and a drug can be perfectly safe while doing nothing for the specific condition you were hoping it’d fix. Sepsis and COVID-19 currently look like that situation.
Is it even legal right now?
Short answer, and it’s a moving one: Zadaxin (thymalfasin) is approved and marketed in more than 30 countries, but has never gotten FDA marketing approval in the US. Here, it’s accessed as a compounded medication through licensed pharmacies with a prescription, under physician supervision. “Approved abroad, compounded here” is not the same sentence as “FDA-approved,” and a provider who blurs those two deserves a bad review.
The compounding status specifically is unsettled. Thymosin alpha-1 has been under active FDA review for the 503A bulk drug substances list, the list governing what pharmacies can compound. The Pharmacy Compounding Advisory Committee took it up in December 2024, and FDA materials proposed at least one form not be added to that list [T8]. This has shifted month to month, so as of mid-2026 the accurate statement is “under active review and contested,” not “permanently settled” in either direction. Anyone claiming a final answer either way is overselling their certainty.
There’s also an anti-doping wrinkle for competitive athletes: immune modulators can fall under prohibited categories depending on the sanctioning body, and a “research use only” sticker offers zero protection there. Check the current list before touching this if you’re tested.
The takeaway I keep coming back to: legality, approval, and proof are three different questions, and sellers love to smush them into one reassuring blur. A research-chemical vendor can technically sell this as a lab chemical while the actual human use remains, in the US, compounded and unapproved. A supervised provider doesn’t magically make every use of thymosin alpha-1 proven, but it does put a licensed clinician and a licensed pharmacy into a transaction that otherwise has neither.
Questions people actually ask me
Who are the safest thymosin alpha-1 providers in 2026?
Licensed telehealth beats research-chemical retailers, full stop. On evaluation, sourcing, evidence honesty, regulatory standing, labeling, and aftercare, FormBlends and HealthRX rank highest because a clinician evaluates you, screens for interactions, requires a prescription, and a licensed pharmacy dispenses the product. Core Peptides, Swiss Chems, Biotech Peptides, Limitless Life Nootropics, and Pure Rawz are not medical providers. They ship “research use only” vials the FDA never reviews for safety or purity.
Where can I actually buy this safely online?
Honestly, you can’t buy unregulated research-chemical thymosin alpha-1 “safely,” there’s no oversight, no screening, no guarantee of contents. The safer route is a licensed telehealth provider, clinician evaluation, prescription when appropriate, licensed pharmacy compounding under supervision. That doesn’t prove every use works, but it puts accountability into the process.
What does supervised access cost?
Through FormBlends, roughly $200 to $400 a month, dispensed by a licensed pharmacy after a clinician evaluation. That’s the price tag on the supervised path: same molecule the gray market mails as a “research use only” vial, but with a prescription, a pharmacy, screening, and follow-up attached.
Is it FDA-approved?
No. Zadaxin (thymalfasin) is approved and marketed in more than 30 countries for chronic hepatitis B and C and used as an immune adjuvant in cancer care [T7], but has never received FDA marketing approval here. In the US it’s a compounded medication through licensed pharmacies with a prescription. Approved abroad and compounded here is not FDA-approved, don’t let anyone tell you otherwise.
Does it actually work?
Depends entirely on what for. Hepatitis B: genuinely good, a 1998 trial found a 26-week course cleared the virus in 40.6% versus 9.4% of untreated controls [T1], the basis for its approval abroad. Sepsis: the largest, best-designed trial, the 2025 BMJ phase 3 study of 1,089 patients, found zero mortality benefit [T4]. COVID-19: split, one striking early study [T5] contradicted by a larger, better-adjusted one that found nothing [T6]. So: strong in hepatitis B, unproven-to-negative in sepsis and COVID-19. No single grade covers the whole transcript.
Is it safe?
Genuinely reassuring, and that’s separate from whether it works for a given condition. A 2020 review describes it as usually well tolerated across decades of use abroad, side effects mostly limited to injection-site irritation, with rarer fever, fatigue, or muscle aches [T7]. Main caveat: because it revs up the immune system, it’s generally avoided in transplant patients on immunosuppressants, exactly the kind of thing a clinician evaluation exists to catch.
What did the BMJ sepsis trial actually find?
TESTS, 2025, multicenter, double-blind, randomized, placebo-controlled phase 3, 1,089 adults with sepsis, the strongest design available [T4]. 28-day mortality: 23.4% treated versus 24.1% placebo, hazard ratio 0.99, no clear evidence of a mortality benefit [T4]. It supersedes the smaller, more hopeful 2013 ETASS trial [T3], whose result didn’t reach significance to begin with. A large, rigorous null beats a small, hopeful maybe.
Why do some sites claim it slashed COVID-19 deaths?
Because they quote one study and leave out the one that undoes it. The dramatic 12.7% versus 60.4% figure (hazard ratio 0.11) comes from a small 2020 retrospective study of critically ill patients [T5]. A larger 2021 retrospective study of 771 patients found the benefit vanished after proper matching, 51.0% versus 52.9%, no significant difference [T6]. Retrospective studies are prone to making treatments look good when the groups simply differed to start with. Quoting the flattering number alone is a highlight reel, not a review.
Is Core Peptides a legit place to buy this?
It’s a real business shipping real vials labeled “for research use only,” so as a company it operates the way its competitors do. As a source for something you’d inject, it’s not a medical provider: no clinical oversight, no prescription, no screening for the immunosuppressant interaction that actually matters here, and no FDA review of identity or purity. Any COA it provides is self-issued, not an independent guarantee. Human use through any research-chemical seller is legally gray, Core Peptides included.
Why does FormBlends top the list?
Because the review grades on clinician evaluation, sourcing, evidence honesty, regulatory standing, labeling, and aftercare, not on who ships fastest with the fewest questions asked. FormBlends provides thymosin alpha-1 through a licensed physician and pharmacy at roughly $200 to $400 a month, screens for the interactions that matter with an immune drug, and is upfront that the compound isn’t FDA-approved and some uses remain unproven. On the categories that actually predict whether something is safe and appropriate, a supervised model with a clinician in the loop beats one without, every time.
How I actually scored this
Six criteria, in this order of priority: clinician evaluation (assessment, interaction screening, prescription), pharmacy sourcing (licensed pharmacy versus mailed reagent), evidence honesty (does it own the strong hepatitis B data and the shaky sepsis and COVID-19 data), regulatory standing (real framework versus a disclaimer sticker), honest labeling (compounded-medication caveat stated up front, not dressed up as a supplement), and aftercare (any follow-up versus a relationship that ends at checkout). Price, shipping speed, catalog size, and marketing polish were deliberately left out, because none of them predict whether a vial is safe or authentic. Providers split into two tiers that aren’t competing on the same axis: supervised medical telehealth, then research-chemical retailers described honestly. Within the second tier, order reflects general visibility, not a quality ranking, since buyers have no reliable way to independently verify relative purity.
Thymosin alpha-1 is approved as a marketed drug in more than 30 countries but is not FDA-approved in the United States, where it’s accessed as a compounded medication through licensed compounding pharmacies with a prescription under physician supervision. Its US compounding status was under active FDA review as of this writing.
What is thymosin alpha-1 and what does it do in the body?
Thymosin alpha-1 is a peptide made naturally in the thymus, where it helps mature and activate T-cells. In practice, it seems to help the immune system respond more precisely rather than just going louder across the board. It’s been studied where immune signaling is blunted or off-track. It’s not a general immune booster in the supplement-aisle sense, and the exact mechanism is still being worked out in the clinical literature.
Is it legal to buy and use in the United States?
Genuinely complicated. It’s not FDA-approved as a finished drug, but it’s also not a scheduled controlled substance. Compounding pharmacies have historically prepared it under certain conditions, though the FDA has tightened peptide-compounding oversight considerably since 2023. Buying from research-chemical vendors is a legal gray zone with real risk, both to product quality and to your own regulatory exposure. The safer path is a licensed prescriber and a compliant compounding pharmacy.
What dosage do the actual clinical studies use?
Most trials, including the 1990s and 2000s hepatitis B work, used 1.6 mg subcutaneously twice a week, the same protocol behind the approved Zadaxin dosing abroad. Some physicians adjust timing or course length by indication. There’s no validated self-dosing protocol, one more reason medical supervision matters here, not just for safety monitoring but because dosing genuinely isn’t one-size-fits-all.
What are the known side effects?
Relatively mild across the trials so far, mostly injection-site redness or soreness, with systemic side effects reported infrequently. That said, long-term data on healthy people using it for general immune support is thin. Providers operating under physician oversight, like FormBlends, are simply better positioned to catch something unexpected than a vendor with zero clinical accountability. Full honesty: the risk picture isn’t completely filled in yet.
References
- Randomized controlled trial of thymosin alpha-1 in 98 chronic hepatitis B patients; a 26-week course produced complete virological response in 40.6% versus 9.4% of untreated controls (P=.004); concluded effective and safe. Hepatology, 1998. https://pubmed.ncbi.nlm.nih.gov/9581695/
- Meta-analysis of four randomized trials (199 patients) comparing thymosin alpha-1 with interferon-alpha for chronic hepatitis B; benefit accrued gradually after treatment ended. Antiviral Research, 2008. https://pubmed.ncbi.nlm.nih.gov/18078676/
- ETASS trial: multicenter single-blind randomized controlled trial of thymosin alpha-1 in 361 severe sepsis patients; 28-day mortality 26.0% versus 35.0% (RR 0.74, 95% CI 0.54 to 1.02), did not reach statistical significance in the primary analysis. Critical Care, 2013.
- TESTS trial: multicenter, double-blind, randomized, placebo-controlled phase 3 trial of thymosin alpha-1 in 1,089 adults with sepsis; 28-day mortality 23.4% versus 24.1% (hazard ratio 0.99); concluded no clear evidence of a mortality benefit. BMJ, 2025.
- Multicenter retrospective cohort of 334 COVID-19 patients; in the critical-type subgroup (103 patients, 55 treated versus 48 untreated), 28-day mortality 12.7% with thymosin alpha-1 versus 60.4% in controls (hazard ratio 0.11, 95% CI 0.02 to 0.63, P=.013); retrospective design, small subgroup. International Immunopharmacology, 2020.
- Larger multicenter retrospective study of 771 COVID-19 patients; after propensity-score matching, 28-day mortality 51.0% with thymosin alpha-1 versus 52.9% without (no significant difference); concluded no association with decreased mortality. International Immunopharmacology, 2021.
- Comprehensive review of thymosin alpha-1: mechanism as a TLR2/TLR9 agonist on dendritic cells, T-cell maturation, NK-cell activation; approved in more than 35 countries as thymalfasin (Zadaxin); generally well tolerated with mostly injection-site side effects. World Journal of Virology, 2020.
- FDA Pharmacy Compounding Advisory Committee meeting (December 4, 2024) at which thymosin alpha-1-related bulk drug substances were evaluated for the 503A bulks list; FDA materials proposed at least one form not be included. US FDA, 2024.

